Understanding and estimating tumor fraction from plasma cell-free DNA
Vessel Tutorial - Understanding liquid biopsy results is highly dependent on tumor fraction of the cell-free DNA sample. Without information about ctDNA content from plasma, variant allele frequencies and uninformative testing results are very difficult to interpret.
In this brief tutorial, we will describe the basics of estimation and analysis of tumor fraction from plasma.
Brief background
Liquid biopsy is a non-invasive and simple alternative to surgical biopsies that helps clinicians discover a wide range of information about a tumor through a simple blood sample. Liquid biopsies rely on the detection of circulating tumor cells (CTCs), cell-free DNA (cfDNA), which in patients with cancer includes circulating tumor DNA (ctDNA), RNA, proteins, lipids, and metabolites present in biofluids of patients.
A simple blood draw, a wealth of information
In principle, bodily fluids other than plasma, such as cerebrospinal fluid, urine, saliva, stool, pleural fluid, and ascites, can also be analyzed, but here we are only going to focus on blood and only on cfDNA, as cfDNA profiling is increasingly being used to guide cancer care in the clinic.
I am not working with cfDNA. Why should I care about cfDNA approaches?
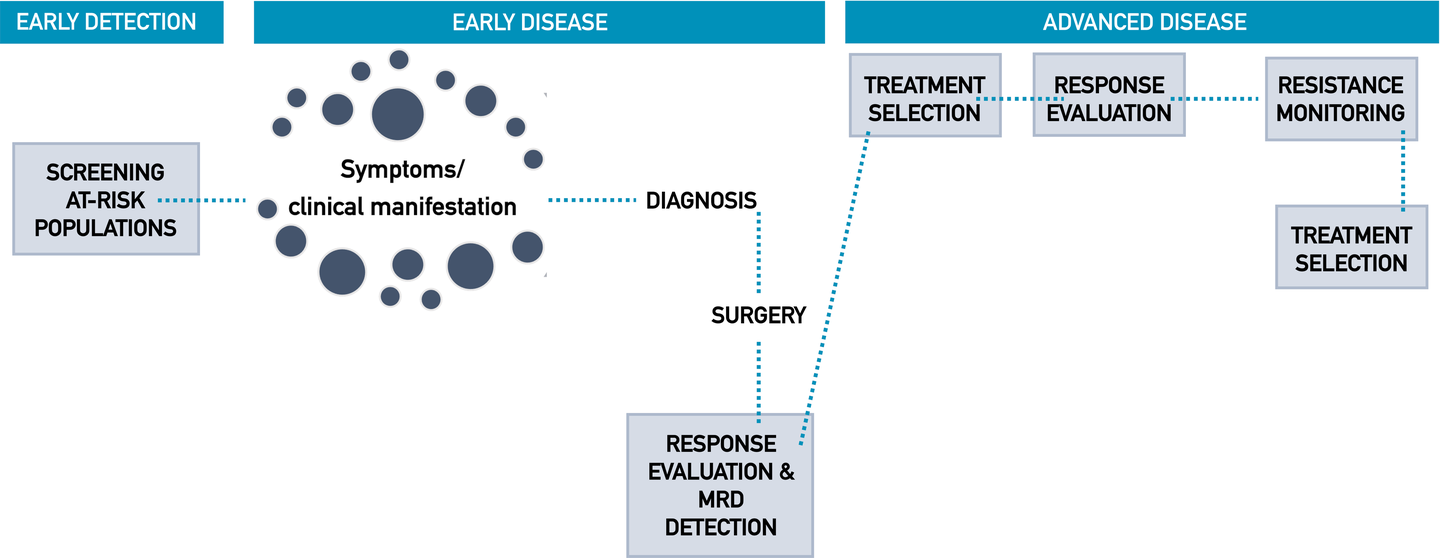
The increasing prevalence of cancer, rising preference for non-invasive procedures, various advantages of liquid biopsy over standard tissue biopsy, favorable government initiatives, and growing public and private interest are factors that are fueling the growth of the cfDNA field. Even though you might not be actively working with liquid biopsy right now at your institution, this approach is going to be central to future precision oncology approaches. Whether you are a pathologist, oncologist, or molecular biologist involved in molecular profiling workflows, getting to know the fundamentals of liquid biopsy will help you navigate the growing field of personalized cancer care and how to integrate these analyses into your existing workflows. Particularly as an oncologist, harnessing liquid biopsy technology will provide you with another tool in your arsenal to help treat patients and guide clinical-decision making, particularly when tissue is inadequate or unavailable altogether. There are numerous established and ongoing efforts to incorporate cfDNA testing throughout the cancer patient journey, owing to many promising emerging NGS-based technologies.
In the future, cell-free DNA testing may be applied to anywhere throughout the patient journey.
Liquid biopsy in a nutshell
Taken from Hasenleithner & Speicher, Molecular Cancer 2022. Please see original text for references.
In addition to their eased access, liquid biopsies may capture the tumoral spatial heterogeneity not observed from traditional single-site biopsy genotyping, as they may enable the detection of DNA shed from both clonal and subclonal sites within multiple metastatic lesions. An array of studies has established the general concordance between aberrations detected in ctDNA and tumor tissue, ranging approximately between 70 and 90%. Some discordance between mutations identified in primary tumor tissue and ctDNA is to be expected, which can be attributed to tumor heterogeneity or evolution, sampling bias, time lapses between sample acquisition, differences in sensitivity of the sequencing assays applied, or even different sequencing platforms. However, with suitable and validated workflows, the potential applications of ctDNA are far-reaching, including diagnosing cancers earlier than traditional imaging, customizing treatments detected via genotyping, associating DNA levels with response to treatment, identifying mechanisms of resistance to therapies and measuring minimal residual disease after treatment. As new evidence of analytical validity, clinical validity as well as utility continues to accumulate for these applications, strategies and requirements for the integration of ctDNA analysis workflows into clinical oncology programs are taking form.
Some basics about cfDNA and ctDNA from the plasma of patients with cancer
In patients with cancer, the cfDNA in plasma is derived from both tumor and normal cells. The majority of DNA in the bloodstream originates from “healthy” white blood cells, with lower amounts of apoptotic or necrotic cancer cells releasing their ctDNA into the circulation. Other DNA populations originate from cells of the tumor microenvironment as well as other non-cancer cells, such as endothelial and immune cells from various parts of the body. For a deeper dive into what is currently known about the biology and release of cfDNA, check out this comprehensive work (PMID: 32359482). However, what you really need to know is that if you analyze DNA taken from a liquid biopsy, the tumor signal that you want to detect (ctDNA) is masked by the signal from the DNA of other healthy cells. Furthermore, the amount of ctDNA that lands in the bloodstream is influenced by many factors. For example, smaller, earlier-stage tumors shed less DNA into the circulation and the amount of shedding differs across tumor types. This means that tumor-derived DNA is only a small fraction of the DNA harvested from the bloodstream, which of course has implications for which assay you choose to employ downstream. For more details about this, see Hasenleithner & Speicher 2022.
The factors that influence tumor fraction in plasma
Tumor fraction from plasma, which is defined as the fractional proportion of tumor DNA relative to total cfDNA, is dependent on multiple factors. These primarily include:
Biological factors associated with tumor DNA shedding, such as:
tumor volume and tumor surface area
vascularization
tumor cell growth and death rates
mitotic and metabolic activity
cell morphology
Clinical factors, such as:
tumor type (some tumors are “good” shedders [e.g. CRC], some are “poor” shedders [e.g. RCC])
active tumor proliferation (more aggressive cancers tend to shed more DNA into the bloodstream)
disease stage (localized, i.e. early-stage vs. metastatic, i.e. late-stage)
overall tumor burden
current clinical response (progressive disease, stable disease, partial or complete response to treatment)
Patient-specific factors such as fasting status or physical activity prior to blood collection
Technical/pre-analytic factors such as blood collection tubes, transport, and sample processing
However, it is very important to note here that, at present, not all factors influencing tumor fraction in plasma are currently known. It is very likely that additional factors that influence tumor content will be identified in the future.
Tumor fraction from plasma is critical for understanding and interpreting your results
You can probably begin to appreciate why negative results from liquid biopsy testing need to be interpreted with caution. Failure to detect a genomic alteration from plasma may simply be related to the low tumor fraction represented in plasma (although failure to detect mutations may also be a result/limitation of the selected assay, such as its breadth or sensitivity). Furthermore, if you have access to serial samples, monitoring the changes in ctDNA levels in conjunction with treatment may help you determine if the patient is responding to therapy or not. The tumor content of a sample is especially important when interpreting variant allele frequencies (VAFs) from an NGS report. For these reasons, determining the cfDNA tumor fraction has become an essential feature of cfDNA molecular profiling. Results that are not provided with the tumor fraction of that sample are limited and must be interpreted with caution.
What are the current approaches to measuring tumor fraction from cfDNA?
There are several methods described in the literature or those that are currently in commercial use to derive tumor fraction. Click on the name of the approach to direct you to the associated literature/source. Here, we will briefly list some examples, but will go into detail about two main approaches used both in research and the clinic.
See you inside. Members have full access to this document
Your North Star in the Transformation of Precision Oncology
See you inside. Members have full access to this document
Your North Star in the Transformation of Precision Oncology
Consider applying if you want to:
Acquire in-depth knowledge and skills, enabling you to excel in your field.
Continuously improve and stay relevant in your career through regular training and development opportunities, positioning you for career advancement
Connect, network, and collaborate with like-minded professionals, gaining unique insights and opportunities that are only available to members of this community.